Structured Abstract
Background:
Chronic kidney disease (CKD) is associated with substantial morbidity, mortality, and cost. CKD is associated with decreased patient quality of life (QOL) and increased caregiver burden. Peer mentoring (PM) improves activation of patients to participate in their own care and multiple outcomes in various chronic diseases. The effectiveness of a peer-led CKD intervention on patient QOL, patient activation, and caregiver burden has not been previously studied.
Objectives:
We conducted a randomized clinical trial to test the effectiveness of face-to-face (FTF) and online mentoring by trained peers, compared with usual care, on CKD patients' QOL, patient activation, and caregiver burden.
Methods:
We randomly assigned 155 patients with CKD and 86 caregivers to receive 6 months of intervention in 1 of 3 groups: (1) FTF PM, (2) online PM, and (3) textbook-only group who received an informational textbook about CKD. Peer mentors were patients with stage 4 or 5 CKD, ≥18 years of age, or caregivers of patients with CKD, ≥18 years of age. Candidates for PM received formal training through 16 hours of instructional sessions facilitated by patients, caregivers, and health care professionals. Upon successful completion of the training, each PM candidate was designated a certified peer mentor. Participants in all 3 groups received a textbook that contains detailed information about kidney disease. Participants assigned to FTF intervention groups received 6 months of PM. Participants assigned to the online intervention group also received 6 months of PM through a secure password-protected interactive online platform. At baseline, 12 months, and 18 months, the patients completed the Kidney Disease Quality of Life-36 (KDQOL-36) instrument and the Patient Activation Measure (PAM) survey. Caregivers completed the Zarit Burden Interview (ZBI). The primary outcomes were (1) improvement in QOL and (2) decreased caregiver burden. The secondary outcome was improved patient activation as measured by PAM. The primary analyses were by intention to treat (ITT). We applied repeated-measures analysis of variance with a linear mixed-effects model to estimate time-related changes in outcome measures for each of the groups over the study period. We conducted exploratory analyses including interaction terms in the statistical models to investigate heterogeneity of treatment effects (HTEs).
Results:
In our ITT analysis, we analyzed 52 patients in the FTF PM group, 52 patients in the online PM group, and 51 patients in the textbook-only group. Compared with baseline, online PM was associated with improved scores in Effects of Kidney Disease (EKD) (P = .01), Burden of Kidney Disease (BKD) (P = .01), Symptoms and Problems of Kidney Disease (P = .006), Short Form-12 (SF-12) Physical Composite Summary (PCS) (P = .001), and SF-12 Mental Composite Summary (MCS) (P = .0001). Compared with baseline, there were no statistically significant changes in KDQOL-36 domain scores in the FTF PM group and the textbook-only group.
For employed participants, exploratory subgroup analyses showed larger effects of FTF PM on increased EKD (P = .002) and BKD (P = .04) scores, and larger effects of online PM on increased EKD score (P = .02), all relative to the study population as a whole. We found a positive effect of “not employed” status on the association between online PM and increased PCS score (P = .01). We also found a positive effect of male sex on the association between online PM and increased MCS score (P < .0001).
Online PM was associated with increases in PAM score from baseline to 18 months (P = .0001). Compared with baseline, no statistically significant changes were found in PAM scores in the FTF group and the textbook-only group.
Exploratory analyses showed that male (P < .0001) and married (P = .003) participants had larger effects of online PM on increased PAM scores. Female (P = .01) and not married (P = .03) participants had larger effects of FTF PM on increased PAM scores, all relative to the study population as a whole.
In our ITT analysis, we analyzed 29 caregivers in the FTF PM group, 29 caregivers in the online PM group, and 28 caregivers In the textbook-only group. Compared with baseline, online PM was associated with a statistically significant decrease in the ZBI score (SE, −3.44; CI, −6.31 to −0.57; P = .002) with no HTE from any of the demographic variables. Compared with baseline, there were no statistically significant changes in ZBI score in the FTF group and the textbook-only group.
Conclusions:
Compared with baseline, online PM was associated with increased scores in 4 domains of the KDQOL-36 and PAM among patients with CKD. We detected HTE response for the effects of employment, sex, and marital status. Compared with baseline, online PM was associated with decreased burden of care among caregivers of patients with CKD. No statistically significant changes from baseline were found in domain scores of KDQOL-36, patient activation scores, or caregiver burden scores among the FTF PM and textbook-only groups.
Limitations:
The study was limited to English-speaking participants with computer literacy and internet access.
Background
Chronic kidney disease (CKD) and end-stage renal disease (ESRD) are significant global health problems. In 2016, the incidence of ESRD in the United States was 124 675 people, and the prevalence reached 726 331, among the highest rates in the world.1 In addition to substantial mortality, morbidity, and cost, CKD has significant negative effects on quality of life (QOL)2,3 that is, in turn, correlated with mortality among CKD patients.4
CKD is a general term for a variety of disorders that affect the structure and function of the kidneys. CKD is characterized by kidney damage, as defined by either abnormal urinary albumin excretion or decreased kidney function, or both, for >3 months. Based on severity of reduction in kidney function, CKD is classified into 5 stages. The complications and chance of progression to the need for kidney replacement therapy (dialysis or transplant) are more likely in severe CKD (stages 4 and 5). Patients with stage 5 CKD, who require kidney replacement therapy for continued survival, are defined as having ESRD.5,6 Patients with stage 1 or 2 CKD progress to more advanced stages at approximately 0.5% per year, and patients with stage 3 or 4 disease progress to stage 5 or ESRD at a rate of 1.5% per year.7
Patient Information Needs
Providing CKD patients with information results in patient-centered care, alleviating anxiety, enabling the individual to cope, facilitating awareness, and improving self-management adherence.8,9 Educating patients with CKD is associated with improved outcomes and is recommended as an area of priority in systematic reviews, professional guidelines, and consensus conferences involving professional societies, providers, patients, and stakeholders.10-18 In response to these recommendations, education programs have been developed.
Despite these educational programs, however, studies have highlighted suboptimal understanding of CKD and its treatment options by patients,19,20 and significant gaps have been identified in desired and provided information.21 Standard CKD eeducational programs are based on information perceived by professionals as important. Information is presented late and often immediately before treatment initiation,22 not allowing time for understanding, engagement, and informed decision-making by patients and caregivers.23,24
A systematic review explored the evidence on the information needs of patients with CKD.25 Some areas that were identified included function of kidneys and manifestations of kidney failure26-28; how progression of kidney disease can be prevented28; unbiased information about the advantages and disadvantages of different treatment options9,27-33; questions about lifestyle, social relationships, networks, activities, and commitments31,32,34-37; information about diet, medications, and their purposes and adverse effects8,27-29,32-34,36,38; rationale for tests, significance of abnormal tests, their relationship with symptoms, and what patients can do when they are informed about abnormal values28,29; coping with consequences of a failed transplant32; how to identify additional support36,38; potential impact of CKD and its treatments on physical appearance29,32,34,37; information about the possibility of death as a result of refusing treatment37; and the realistic chances of survival.21,27,32,37
Findings from another systematic review indicated that patients with CKD value knowledge that allows them to regain some control in their lives, to cope with illness, and to alleviate anxiety stemming from uncertainty.39 Well-informed patients are better able to be engaged in their care; lack of knowledge is a source of anxiety and stress. Another important finding from this systematic review was that patients place value on relationships and being part of social networks of family, friends, health care staff, and other patients. These networks provide strength and support.39
Family members of patients with CKD, in addition to the practical aspects of being caregivers (eg, transportation), often provide psychological and cognitive support during the decision-making process. Caregivers are likely to broaden the range of considerations influencing decisions about kidney replacement therapy.40,41 CKD and its treatment influences the patients' role and function within the family and affects the entire family.32,34 In their role as caregivers, family members often experience stress, depression, and poor QOL. Yet their needs are often neglected and underprioritized, despite the obvious impact they may have on patient-centered care.
Important Factors in Educational Programs and Peer Support
Educational programs addressing factors that patients with CKD and their families consider important are likely to facilitate choice of treatment congruent with patients' and families' wishes and values.40 Such education will improve the family members' understanding of the risks and benefits of various treatments, facilitating discussions about expectations and goals of care. Knowledge about goals of care will help prepare family members for the practical aspects of the burden related to various treatment options, engaging them in the patient's care. Patients have also expressed concern about the devastating impact of CKD on caregivers and have suggested assessment of caregiver burden and improvement of support for caregivers among research priorities.42
Interactive educational interventions that involve individuals and groups may improve knowledge, activation to participate in care decisions, and patient outcomes.14 Peers with experience in managing their CKD may be in a unique position to communicate knowledge and confidence to a recently diagnosed patient in a more personalized manner. Patients with CKD have indicated the desire to meet other patients.21,30,32,36,38 They are interested in the experiences of others, not as a source of medical information27 but to discuss ideas on how to cope.30 Comparing themselves with their peers will reassure them of their own situation and will reduce their sense of isolation.31,43 There are at least 2 differences between a patient navigator program and peer mentoring (PM): First, a patient navigator is not necessarily a peer with a similar set of experiences; second, the primary goal of patient navigator programs is to overcome barriers for access to care, whereas PM has multiple additional goals, including sharing experiences, discussing coping mechanisms, and communicating knowledge and confidence.
Heisler proposed several models of peer support.44 These models include professional-led group visits; peer-led self-management training; peer coaches; community health workers; support groups; telephone-based peer support; and web- and email-based programs. The effectiveness of PM has been attributed to the nonhierarchical reciprocal relationship created by sharing similar experiences.45 Relationship-centered mentoring by trained peers is an effective strategy that provides individualized patient-centered information. PM has been shown to lead to improvements in activation of patients to participate in their own care, confidence in care, and multiple outcomes in various chronic diseases.46-53
Patient and Family Partner Program
Since 2004, the Kidney Foundation of Central Pennsylvania (KFCP) has operated a comprehensive patient engagement and empowerment program (Patient and Family Partner Program [PFPP]). Through the PFPP, trained patients with CKD and their family partners serve as volunteer peer mentors to other patients with CKD and their caregivers to help them engage successfully in their own care.54 Information about the impact of trained mentors on the care of patients with CKD is lacking. More specifically, a peer-led CKD intervention has not been assessed for its impact on patient activation, patient QOL, and caregiver burden.
To address this issue, we examined the impact of a formal PM program on patient QOL, patient activation, and caregiver burden among patients with CKD and their caregivers. Knowledge gained from this randomized clinical trial (RCT) can potentially be extrapolated to other chronic disease states. We hypothesized, as depicted in , that a formal structured mentoring program, based on information needs of patients and caregivers, would lead to improved patient QOL (aim 1) and decreased caregiver burden (aim 2). We also hypothesized that such educational programs would lead to activation of patients to participate in their own care (aim 3).
The specific aims of this RCT were as follows:
To determine whether PM leads to improved QOL among patients with CKD.
To determine whether PM leads to improved caregiver burden among caregivers of patients with CKD.
To determine whether PM leads to improved patient activation among patients with CKD.
Patient and Stakeholder Engagement
Patients, caregivers, and other stakeholders were involved in various stages of the study. The PFPP, initially named Patient-Partner Program (PPP), was envisioned by a kidney transplant recipient who was a registered nurse and a member of the KFCP board of directors.55 She partnered with a renal social worker and a transplant coordinator to develop a PM program for patients with ESRD. Following a thorough literature and internet search, as well as personal contacts, the founding group developed a preliminary curriculum for the PPP. Based on input from renal physicians and social workers, the curriculum and the program has undergone periodic modification.55 Acknowledging the vital role of caregivers and family members in the care of patients with CKD, the founding group, consisting of a patient, a renal social worker, and a transplant coordinator, changed the name of the program to PFPP in 2011.
By 2011, approximately 80 mentors and >200 mentoring partnerships had been established. Review of mentor and mentee evaluations pointed toward relative success of the program. Mentored patients noted improved adherence with treatment and overall satisfaction with the improved adherence; mentors reported satisfaction with their roles; and both groups perceived the bonding experience as a very positive influence.
To assess the performance of the program and to discuss its future direction, we convened a focus group in August 2011. Participants in the focus group included the 3 original founders (a patient, a renal social worker, and a transplant coordinator), a dialysis patient, spouse of a transplanted patient, a social worker, director of the KFCP, the program coordinator, and the medical director of the PFPP. The current study is congruent with the 2 main themes identified in the focus group as the proposed goals of expansion of the PFPP: (1) Creating an online version of the program was proposed as a possible strategy to expand the PFPP to include rural areas; and (2) expanding the PFPP to include patients with pre-ESRD was deemed essential to the overall success of the program.
presents the governance of the research team. For this study, the research team organized 3 advisory groups and engaged 3 individual advisors (see the Acknowledgments section) as follows:
Patient and Caregiver Advisory Group consisted of 12 members (7 patients and 5 caregivers) and provided the patients' and caregivers' perspectives about the content of the interventions, strategies for recruiting participants, and interpreting and disseminating findings. We recruited Patient and Caregiver Advisory Group members from among previously trained PFPP mentors, through a general call for volunteers on the KFCP website, and nomination by the KFCP and PFPP program coordinator.
Provider Advisory Group consisted of 12 members and included nephrologists (2), nephrology advanced practice providers (1), primary care providers (1), dialysis social workers (2), transplant social workers (2), dialysis nurses (2), and transplant coordinators (2). The research team identified members of the Provider Advisory Group through professional networks in the community.
Community Advisory Board consisted of the 15-member volunteer board of directors of the KFCP. The membership of the board of directors included patients (2), caregivers (2), community nephrologist (1), academic nephrologist (1), transplant surgeon (1), senior medical director of a major health care network and a primary care physician (1), vice president of another health system (1), dialysis social workers (2), members of the community (3), and an attorney (1). Some board members have been trained as mentors. The Community Advisory Board provided insights for developing the proposed research and oversight during the study. The principal investigator, a member of the board of directors since 2011, presented updates on the project at the quarterly meetings to seek input on recruitment, study flow, evaluation, and dissemination of findings. The Community Advisory Board's partnership with the KFCP board provided an opportunity to present preliminary results at the KFCP annual symposium on kidney disease.
Individual advisors included an experienced renal social worker who was one of the original founders of the PFPP. She is highly regarded in the renal social work community of central Pennsylvania and, to improve recruitment, assisted in the description of the PFPP for potential participants and health care providers. The 2 patient advisors had previously completed training as mentors in the PFPP. Collectively, the 3 advisors provided insight into creating interventions; they particularly assisted in developing the content of the online PM intervention.
In addition to their roles within the advisory groups, patients, caregivers, and stakeholders played key roles in implementing the study. During training of peer mentors, stakeholders delivered parts of the content. The interventions (face-to-face [FTF] and online PM) were carried out entirely by patients and caregivers. Each year, a panel of patients and caregivers who were involved in the study presented updates and their personal experiences at the KFCP annual symposium on kidney disease. During the second year of the study, the Community Engagement Studio, organized by the Penn State Clinical and Translational Science Institute Comparative Effectiveness Research Center, was convened to present results and to explore options for public dissemination.
Methods
Study Overview
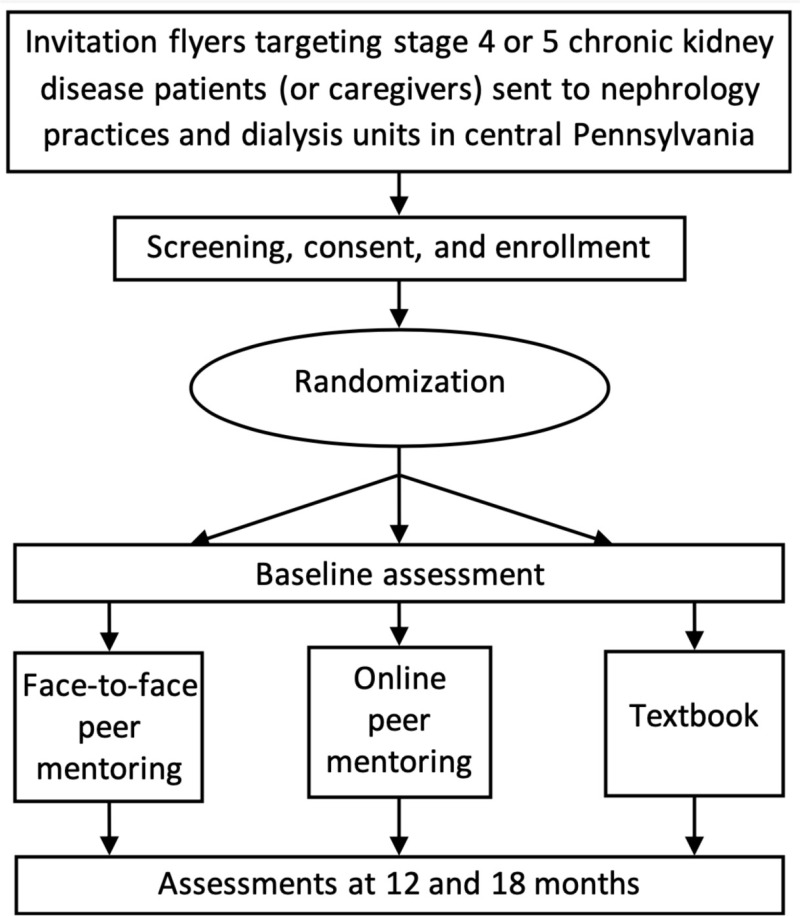
We conducted an RCT to test the effectiveness of mentoring by trained peers on QOL for patients with CKD as measured by the Kidney Disease Quality of Life-36 (KDQOL-36) instrument (specific aim 1), caregiver burden as measured by the Zarit Burden Interview (ZBI) (specific aim 2), and patient activation as measured by the Patient Activation Measure (PAM) (specific aim 3). We randomly assigned patients with CKD and their caregivers into 3 groups: (1) FTF PM plus informational textbook about CKD; (2) online PM plus informational textbook about CKD; and (3) textbook only (participants received the informational textbook about CKD but no PM). We used the PFPP, described earlier, as the mentoring program for the PM intervention groups.
Patients with CKD and their caregivers assigned to FTF intervention groups received 6 months of PM and the informational textbook of the PFPP. Participants assigned to the online intervention group also received 6 months of PM through an interactive online platform and the informational textbook of the PFPP. The textbook-only group received the informational textbook of the PFPP to review independently.
At baseline, 12 months, and 18 months, the patients completed the KDQOL-36 instrument and the PAM survey; the caregivers completed the ZBI. presents the study design.
Study Setting
We conducted the trial among patients with CKD and their caregivers residing in 1 of the 28 counties served by the KFCP. The wide recruitment area included urban and rural areas, all racial and ethnic categories, and all socioeconomic levels. The Pennsylvania State University College of Medicine IRB approved the research protocol. We registered the protocol with ClinicalTrials.gov (identifier NCT02429115).
Participants
The study population came from dialysis units and nephrology practices in central Pennsylvania. We recruited participants from among patients with stage 4 or 5 CKD, or caregivers of patients with CKD. Inclusion criteria included the following: (1) patients diagnosed with stage 4 or 5 CKD by a physician, or caregivers of a patient with CKD; (2) at least 18 years of age; (3) able to read and write in English at the eighth-grade level; (4) having access to a computer with internet and email capability; and (5) willing to participate. Exclusion criteria were the following: (1) participation in previous PM for CKD; (2) inability to provide consent; (3) currently an inmate; and (4) physical condition preventing active participation in mentoring program as determined by primary nephrologist.
We sent information packets about the program to dialysis units and nephrology practices asking renal professionals to distribute them among patients and caregivers. The principal contact person in each practice was the social worker. The packets included an introduction to the program and an application form. A substantial number of the renal professionals, particularly renal social workers within the area served by the KFCP, have been familiar with the PFPP since its establishment. The program coordinator contacted all the nephrology practices and dialysis units every quarter to provide them with information about the program. The program coordinator, research coordinator, or both traveled to the dialysis units and provided information about PFPP and recruitment flyers to be distributed among patients and their caregivers. The flyers encouraged patients and their caregivers who might be interested in exploring being matched with a mentor to contact their social worker, the program coordinator, or the research coordinator.
Following informed consent, candidates underwent permuted block randomization with 1:1:1 allocation into “FTF PM,” “online PM,” and “textbook only.” The investigators did not have access to the identity of the participant assignment until they confirmed that the participant was eligible for enrollment.
Recruitment occurred continuously until we achieved the target sample sizes. In the initial screening questionnaire, we asked the potential candidates who declined to participate to indicate reasons for declining. To improve retention, we compensated participants with a $50 stipend for the baseline assessment and each of the follow-up assessments (ie, 12 months and 18 months) for a total of $150 per participant.
Interventions and Comparators or Controls
The description of the intervention follows the Template for Intervention Description and Replication (TIDieR) checklist developed by Hoffmann et al.56 The existing training of peer mentors in the PFPP involved the following: Mentors were patients with stage 4 or 5CKD, ≥18 years of age, or caregivers of patients with CKD, ≥18 years of age. Candidates for becoming a mentor received formal training through 16 hours of instructional sessions facilitated by patients, caregivers, and health care professionals. Based on feedback from participants and the board of directors of the KFCP, the curriculum committee revised the training program to include new topics, such as understanding mentees' choices, special needs of older adults, special needs of children and adolescents, and the effect of CKD on the family. The final curriculum is shown in Appendix A.
Upon successful completion of the training, each peer mentor received a certificate from the KFCP as a certified mentor. Key features of a successful PM program include sufficient training and ongoing support for peer mentors, regular opportunities for mentors to receive additional training, and appropriate recognition for their efforts.44 Recognizing the importance of continuing education following the initial training, we conducted refresher courses on a quarterly basis. These sessions, which the program coordinator facilitated, featured discussions among mentors about their actual experiences and a focused review of communication skills. Each mentor was required to attend at least 1 refresher course per year to maintain certification.
The 3 interventions were (1) FTF PM, (2) online PM, and (3) textbook only. Participants in all 3 groups received a copy of the PFPP textbook that contains detailed information about kidney disease and was prepared targeting an eighth-grade reading level. The choice of interventions emerged following a review of mentor and mentee evaluations and a focus group discussion involving dialysis and transplant patients, renal social workers, the director of the KFCP, the PFPP program coordinator, and the PFPP medical director.
We mounted the online intervention based on the focus group discussions and evidence that web-based peer support is a potential alternative to FTF mentoring, particularly for populations with limited ability to travel and for regions with limited resources. Online peer support groups have enhanced the care of diabetes.57,58 For example, Zrebiec evaluated a web-based educational and emotional resource for patients with diabetes and their family members at Joslin Diabetes Center in Boston, Massachusetts. Over 74 months, 74% of all respondents rated participation in the discussion board as having a positive effect on coping with diabetes, and 71% rated participation as helping them to feel more hopeful.59 Additional evidence supports the effectiveness of online chronic disease self-management.60
FTF PM Group
Individual mentees had the choice of meeting their mentor at a location preferred by the mentee. If the pair decided on a lunch meeting, KFCP provided reimbursement. The frequency of contact by a mentor was weekly by telephone and monthly for an FTF visit. At the end of each month, the mentor presented the log of the meetings to the program coordinator. The partnership was maintained for 6 months. The program coordinator maintained records of adherence by mentor-mentee pairs.
Online PM Group
Mentors and mentees communicated using a secure password-protected interactive online platform, which consisted of a web-based bulletin board designed specifically for this study. We developed the contents of the online PM program according to the themes that emerged from qualitative interviews and discussions with experienced peer mentors, patients, caregivers, and health care professionals. Each enrolled participant assigned to the online PM group was matched with a mentor based on treatment modality (for caregivers, this was the treatment modality of the patient for whom they were the caregiver). All communications between mentors and mentees were online.
Following initial introductions, the mentors initiated the discussion thread by presenting an overview of the program. The mentors and mentees also reviewed mutual goals and expectations at the time of initial communication. Mentors encouraged mentees to familiarize themselves with the textbook and to post any questions or update their status using written statements or mood and symptom icons. The mentors responded to questions or posted a query about the updated status. The mentors sent a weekly reminder email to the mentees to log on to the website to review posted contents and to post a weekly action plan, as well as any problems they wished to discuss with their individual mentors. The frequency of contact by mentors was weekly or more frequently as initiated by the mentees. The program coordinator maintained regular contact with the mentors and mentees and closely monitored the frequency and content of the interactions to ensure appropriate communication, to correct inaccurate information posted by participants, and to direct the mentees to their care providers in situations requiring medical intervention. The partnership was maintained for 6 months. The program coordinator maintained records of adherence by mentor-mentee pairs.
Textbook-Only Group
This group received the textbook with instructions to ask questions of the care providers. The textbook contains information about the structure and function of the kidneys, causes of kidney failure, dietary considerations in kidney disease, and modes of treatment for CKD. Adherence to the review of material was by self-report.
Study Outcomes
Primary Outcomes
The primary outcome for specific aim 1 was improvement in health-related QOL (HRQOL) as measured by the KDQOL-36 instrument from the Rand Corporation. This 36-item instrument was developed as a self-reported HRQOL tool designed specifically for patients with CKD.61 The KDQOL-36 combines the SF-12 and 24 domains specifically targeted to kidney disease. The SF-12 yields the Physical Composite Summary (PCS) and the Mental Composite Summary (MCS). The domains specifically targeted to kidney disease comprise 3 scales: the 4-item Burden of Kidney Disease (BKD), the 12-item Symptoms and Problems of Kidney Disease (SPKD), and the 8-item Effects of Kidney Disease (EKD). The instruments are scored on a scale of 0 to 100, with higher numbers indicating better HRQOL.62
The KDQOL-36 has been validated among patients with CKD with predictive value for several outcomes, including survival; it is the most widely used measure of HRQOL in the nephrology literature.62-71 A single KDQOL-36 Summary Score was recently proposed by Peipert et al.73 In this report, we present the results in the form of separate component summaries of the KDQOL-36.
The primary outcome for specific aim 2 was caregiver burden as measured by the ZBI. Despite the increasing awareness of the burden and adverse effects of CKD on caregivers, high-quality evidence is lacking about the effect of information or support interventions on the psychosocial well-being of caregivers.74 The ZBI is a self-administered questionnaire of 22 items that measures the impact of caregiving in psychological, physical, and social domains. The items are rated on a 5-point Likert scale.75 The total score is calculated from 0 to 88; the higher the score, the heavier the burden.76 The ZBI has been used to measure caregiver burden among caregivers of patients undergoing dialysis77 and for numerous other chronic disease states.78-84 Higher ZBI scores are associated with depression and anxiety.85
Secondary Outcome
The secondary outcome was improvement in patient activation (specific aim 3) as measured by the PAM, a valid and reliable instrument to measure activation of patients to participate in their own care. The PAM was developed based on qualitative research, Rasch analysis, and classical test theory.86 The instrument is a participant-completed questionnaire that yields a continuous activation score ranging from 0 to 100, representing patients' positions along a multistage hierarchical process of activation. Activated patients identified by higher PAM scores are more likely to benefit from interventions designed to improve their health-related knowledge, skills, motivation, and behaviors.
The PAM is a well-validated tool for assessing patient activation and the impact of such activation on outcomes among individuals with various chronic diseases, such as inflammatory bowel disease87 and multiple sclerosis.88 The PAM was also validated as a measure of patient activation and adherence to physical therapy for individuals undergoing elective spine surgery, as reflected in attendance and engagement.89 The high reliability estimate of PAM (Cronbach α = .91) maintains precision across sex and age groups90 and geographic locations.91-93 Higher PAM scores are associated with better self-management health behaviors such as adherence to medication regimens and other health behaviors, higher satisfaction, better QOL, and improved physical and mental functioning.90,94,95 Initially developed as a 22-item instrument, the 13-item short version of the PAM was shown to have similar validity to the original version.91,96
Sample Size Calculations and Power
Sample Size for Patients
The primary outcome for specific aim 1 was improvement in KDQOL-36 score. A 10-point change in the components of the KDQOL-36 was associated with significant changes in clinically relevant outcomes.72 Considering a minimally clinically important difference (MCID) of 10, a mean of 63, an SD of 13 (Mapes et al72), an α of .05, and a comparison of 3 means, we expected that a sample size of 39 patients per group would yield a statistical power of 0.8. Assuming a dropout rate of 15%,60 the total target sample size was 132 patients (44 for each of the 3 study groups).
Sample Size for Caregivers
Change in ZBI score was the primary outcome for specific aim 2. We computed the number of participants needed using data from a study assessing burden among caregivers of patients undergoing peritoneal dialysis, in which the mean combined caregiver burden score (±SD) was 12.5 ± 8.7 (Shimoyama et al77). For our study, we selected 1 SD as the MCID. Assuming an effect size of 1 SD, an α of .05, and a comparison of 3 means, we expected that a sample size of 23 would yield a statistical power of 0.8. Our target total sample size was 84 caregivers (28 for each of the 3 study groups) to adjust for a dropout rate of 15%.
Time Frame for the Trial
According to individual studies,98,99 a systematic review of 15 studies,100 a qualitative synthesis of 25 studies,101 and a review of 11 studies,102 the effective duration of PM for chronic diseases has ranged from 6 weeks to 2 years. Based on these reports, we selected 6 months as the length of intervention. Sustainability of any QOL effect has ranged from 3 months103 to 18 months.104 We chose 12 months postenrollment (6 months after completion of intervention) for quantitative follow-up assessments. To evaluate any sustained intervention effect, we repeated assessments at 18 months.
Data Collection and Sources
Quantitative data for this RCT included responses to self-administered survey instruments delivered by regular mail. We transferred electronically coded data into a secure database that was constantly password protected with no linkage to any personal identifiers in this file. We used statistical alterations to ensure that individuals could not be identified through any study data set.
To maximize follow-up rates, the program coordinator used email messages and telephone calls to remind the participants to complete the surveys. Participants received monetary compensation for their time. The program coordinator contacted participants and their respective social workers to determine reasons for withdrawal or loss to follow-up.
Analytical and Statistical Approaches
The independent variable was allocation to the FTF PM, online PM, or textbook-only groups. Our 3 dependent variables (outcomes) were the following: scores on the KDQOL-36 (aim 1), ZBI (aim 2), and PAM (aim 3). The outcome variables were continuous and measured at 3 time points (baseline, 12 months, and 18 months). Covariates included demographic measures (age, sex, race/ethnicity, marital status, attended or completed college, employment status, and rural vs urban location). We used repeated-measures analysis of variance within the context of a linear mixed-effects model to estimate time-related changes in scores. The analyses included values of all 3 measurements (baseline and subsequent follow-ups) of the outcome variables.
The data source for covariates other than rural/urban location was predominantly participant self-report. The data source for rural vs urban location was based on the address and rural-urban commuting area code.105 We used type 3 fixed effects to test the statistical significance of each of the demographic variables.
To minimize the limitations of self-report data, we ensured that the questions were clearly worded and that we collected data at time of enrollment and at each follow-up visit (Appendices B and C). Analyses were by intention to treat (ITT). We computed descriptive statistics for all variables. We assumed that missing data would occur at random. None of the variables had >10% missing data. The statistical analyses based on restricted maximum likelihood estimation for the linear mixed-effects model allowed for valid and unbiased conclusions in the presence of data that are missing at random.
We had insufficient evidence to support a priori hypotheses about heterogeneity of treatment effects (HTEs), and thus we planned no hypothesis-driven HTE analyses. To investigate HTEs, however, we conducted exploratory analyses by including interaction terms, such as employment status, in the statistical models. We also pursued exploratory subgroup analyses (age, sex, race/ethnicity, education, employment, and rural/urban residence). We investigated reasons for participants' dropout. We used SAS, v.9.4 (SAS Institute, Inc) for data analysis.
Changes to the Original Study Protocol
We requested a 10-month no-cost extension to allow for assessment of all outcomes at 18 months; this let us perform analyses beyond the initial 12-month assessment in our original milestones. The extension facilitated evaluating persistence of the effects of the interventions on the outcomes.
In the original protocol, we had included 3 primary outcomes. We subsequently changed the patient activation to a secondary outcome. We added “participation in previous peer mentoring for CKD” and “physical condition preventing active participation in mentoring program” to the exclusion criteria.
Results
Patient Populations and Demographics
The CONSORT diagram () describes the flow of patient participants through the study interventions. We assessed 236 patients with stage 4 or 5 CKD for eligibility. We excluded 81 patients. Of these, 73 did not meet inclusion criteria (no internet access, n = 61; previous mentoring for CKD, n = 12), and 8 eligible patients declined to participate after receiving more information about the study because of the perceived burden of participating in the study.
Using permuted block randomization with 1:1:1 allocation, we randomly assigned 155 patients to 3 groups. All patients began participation in the interventions and completed the baseline assessment. Of these, 117 patients completed the interventions and the 18-month assessment. Assessments consisted of completion of the KDQOL-36 instrument (specific aim 1) and PAM (specific aim 3).
presents the baseline characteristics of the patients. Baseline demographic characteristics did not significantly differ statistically among the 3 groups (Appendix D documents the details of patients' demographic characteristics).
Among the FTF group, 45 patients completed the allocated intervention and the 12-month assessment; 40 patients completed the 18-month assessment. Among the online PM group, 45 patients completed the allocated intervention and the 12-month assessment; 42 patients completed the 18-month assessment. Among the textbook-only group, 40 patients completed the allocated intervention and the 12-month assessment; 35 patients completed the 18-month assessment. We included 117 patients in the final analyses.
Patient Outcomes: Aims 1 and 3
The key outcomes for aim 1 and aim 3 were KDQOL-36 score and PAM score, respectively.
Aim 1: KDQOL-36 scores: main analyses
In , we document the unadjusted mean scores of the EKD, BKD, SPKD, and SF-12 PCS and MCS of the KDQOL-36 in the 3 groups at baseline, at 12 months, and at 18 months.
shows the changes in mean (∆) scores from the KDQOL-36 over the study period. We note the following findings:
FTF PM was not associated with any significant change in the mean scores of any of the KDQOL-36 domains at 18 months.
Among the textbook-only group, no significant changes were found in the mean scores of any of the KDQOL-36 domains at 12 months or 18 months.
shows changes in the scores from the KDQOL-36 over the study period, adjusted for demographic variables (race/ethnicity, sex, age quartile, marital status, attended or completed college, employment status, and rural/urban location), using ITT analysis. The slope estimates represent change in scores in standard points over 18 months.
Online PM was associated with a statistically significant increase in 5 slope scores:
EKD score (slope estimate, 4.13; 95% CI, 0.87-7.4 [P = .01]).
BKD score (slope estimate, 5.44; 95% CI, 1.24-9.64 [P = .01]).
SPKD score (slope estimate, 6.00; 95% CI, 3.09-8.91 [P = .006]).
SF-12 PCS score (slope estimate, 2.50; 95% CI, 0.95-4.06 [P = .001]).
SF-12 MCS score (slope estimate, 3.46; 95% CI, 1.78-5.13 [P = .0001]).
Compared with textbook only, online PM was associated with a statistically significant increase in 4 comparisons of slope scores:
In the BKD domain (6.43; 95% CI, 0.27-12.58 [P = .04]).
In the SPKD domain (8.71; 95% CI, 5.35-12.07 [P = .003]).
In the PCS domain (3.20; 95% CI, 0.95-5.48 [P = .01]).
Compared with textbook only, FTF PM was associated with a statistically significant increase in the slope score for the SPKD domain (6.12; CI, 2.62-9.38 [P = .04]).
Aim 1: KDQOL-36 Scores: Subgroup Analyses
We performed exploratory analyses to investigate HTEs. We used type 3 fixed-effects models to identify statistically significance (P ≤ .05) [demographic variable × KDQOL domain score] to include in the multivariable model. Results appear in .
Exploratory subgroup analyses displayed in and (for EKD and BKD, respectively) showed heterogeneity for the effects of being employed on the association between FTF PM and increased EKD (P value of slope estimate = .002) and BKD (P value of slope estimate = .04) scores and the association between online PM and increased EKD score (P value of slope estimate = .02). When comparing FTF PM with textbook only, employment had a positive effect on the difference between the slopes of change of EKD (P value of slope estimate = .02) () and BKD (P value of slope estimate = .03) () in the FTF group vs the textbook-only group. All analyses were by ITT.
In exploratory subgroup analyses shown in , “not employed” status had a positive effect on the association between online PM and increased SF-12 PCS score (P = .01). We also detected a positive effect of “not employed” status on the difference between slopes of change in SF-12 PCS score in the online PM group vs the textbook-only group (P = .04). All analyses were by ITT.
Being male (shown in ) had a positive effect on the association between online PM and increased SF-12 MCS score (P < .0001). We also saw a positive effect of male sex on the difference between slopes of change in the SF-12 MCS score in the FTF PM group vs the online PM group (P = .02) and between slopes of change in SF-12 MCS score in the online PM group vs the textbook-only group (P = .02).
Aim 3: PAM scores: main analyses
Patient activation highlights patients' preparedness and ability to take independent actions to manage their health and care and is a component of patient engagement. An improvement of 4 points in the PAM score is considered an MCID.97 The mean PAM scores in the 3 groups at baseline, 12 months, and 18 months are shown in . The mean baseline scores were not statistically different among the 3 groups.
shows the changes in mean PAM scores from baseline to 12 months and 18 months. Online PM was associated with a statistically significant increase in the mean PAM score at 12 months (∆, 10.5; 95% CI, 4.5-16.6 [P = .0009]).
Online PM was also associated with a statistically significant increase in mean PAM score at 18 months (∆, 11.0; 95% CI, 4.7-17.3 [P = .0008]).
FTF PM and textbook only were not associated with statistically significant changes in mean PAM scores at 12 months or at 18 months.
shows changes in PAM scores from baseline to 18 months adjusted for demographic variables (race/ethnicity, sex, age quartile, marital status, attended or completed college, employment status, and rural/urban location). The online PM group experienced a significant increase in the PAM score in the study period (slope estimate, 5.66; 95% CI, 2.79-8.52 [P = .0001]). The difference between the slopes of the FTF PM PAM score and the online PM PAM score was also statistically significant (SE, −4.70 ± 2.07; 95% CI, −8.79 to −0.62 [P = .02]). The difference between the slopes of the online PM PAM score and textbook-only PAM score was also statistically significant (SE, −5.63 ± 2.12; 95% CI, 1.44-9.83 [P = .01]).
Subgroup analyses: PAM scores: aim 3
We performed exploratory analyses to investigate HTEs. We used type 3 fixed-effects models to identify statistical significance (P ≤ .05) [demographic variable × PAM score] to include in the multivariable model ().
In exploratory subgroup analyses documented in , we detected a positive effect of male sex on the association between online PM and increased PAM score (P < .0001). Female sex had a positive effect on the association between FTF PM and increased PAM score (P < .01). With respect to the comparisons, being male had a positive effect on the difference between slopes of change in PAM score for the FTF PM group vs the online PM group (P < .0001) and between the online PM group and the textbook-only group (P < .0001).
In other exploratory subgroup analyses of marital status (), being married had a positive effect on the association between online PM and PAM score (P = .003). In contrast, “not married” status had a positive effect on the association between FTF PM and increased PAM score (P = .03). “Not married” status also had a positive effect on the association between online PM and increased PAM score (P = .008). In addition, we found a positive effect of “married” status on the differences in slopes of change for PAM score in the FTF PM group vs the online PM group (P = .0008) and in the online PM group vs the textbook-only group (P = .02).
Aim 2: Caregiver Outcomes
The CONSORT diagram in describes the flow of caregiver participants through the study interventions. This focus involves specific aim 2 and completion of the ZBI. We assessed 122 caregivers of patients with stage 4 or 5 CKD for the caregivers' eligibility. We excluded 36 caregivers: 22 did not meet inclusion criteria (no internet access, n = 18; previous mentoring experience, n = 4), and 14 eligible caregivers declined to participate after receiving more information about the study owing to the perceived burden.
We randomly assigned 86 caregivers to the 3 groups. All caregivers completed the baseline assessment and started participation in the interventions. Seventy caregivers completed the interventions and the 18-month assessment. Fifteen caregivers were lost to follow-up before the 12-month assessment, and 1 caregiver withdrew from the trial after completing the 12-month assessment.
documents the primary baseline characteristics of the caregivers. Appendix E presents details of caregiver demographics. Baseline demographic characteristics did not significantly differ statistically across the 3 groups.
Aim 2: Caregiver burden scores
The mean ZBI scores in the 3 groups at baseline, 12 months, and 18 months are shown in . The mean baseline scores did not statistically differ among the 3 groups.
shows the changes in mean scores from the ZBI over the study period.
FTF PM was associated with a statistically significant decrease (improvement) in the mean ZBI score at 12 months (∆, −5.1; 95% CI, −10.0 to −0.2 [P = .04]). FTF PM was also associated with a statistically significant improvement in the ZBI score at 18 months (∆, −7.1; 95% CI, −12.2 to −2.1 [P = .007]). Online PM was associated with a statistically significant improvement in the mean ZBI score at 12 months (∆, −7.1; 95% CI, −13.3 to −0.9 [P = .03]). Online PM was also associated with a statistically significant improvement in the ZBI score at 18 months (∆, −8.4; 95% CI, −14.9 to −1.9 [P = .01]).
shows changes in caregivers' ZBI scores over the study period, adjusted for demographic variables (race/ethnicity, sex, age quartile, marital status, education, employment status, and rural/urban location). ZBI scores decreased significantly in the study period in the online PM group (SE, −3.44; 95% CI, −6.31 to −0.57 [P = .002]). ZBI scores did not significantly change among the FTF PM group or the textbook-only group.
No demographic variables had a significant independent effect on the change in ZBI scores among groups.
Discussion
Key Findings
The findings from this clinical trial support the hypothesis that PM improved some QOL and patient activation scores among patients with advanced (stages 4 and 5) CKD. PM was also associated with improvements in caregiver burden score.
Compared with textbook-only and FTF PM, online PM was associated with improvements in scores for the EKD, the BKD, the SPKD, the SF-12 PCS and the MCS of the KDQOL-36, and the PAM. Online PM was also associated with improved caregiver burden (ie, improved ZBI scores).
Compared with textbook only, FTF PM was associated with improved SPKD scores. FTF PM was associated with improved outcomes after exploratory subgroup analyses, with a positive effect in EKD and BKD scores among employed participants and a positive effect of female sex and unmarried status on PAM scores (see the Treatment Response Heterogeneity section).
Our findings are consistent with studies that have shown effectiveness of online social support networks in improving patient-related outcomes. The use of professionally moderated internet discussion groups and peer-led online interventions has been proposed as a strategy for patient engagement, self-management, information exchange, and support for patients with chronic disease.106-108 Lorig et al109,110 found that an internet-based, peer-led chronic disease self-management program (CDSMP) reduced health care use and improved health-related behavior change, self-efficacy, and satisfaction with the health care system. The effects were similar to results for small-group CDSMP. Other forms of internet-based interventions associated with improved chronic disease management include discussion boards, computer-tailored feedback, and behavioral e-counseling.111,112
Despite the findings just noted, uncertainty persists about the effectiveness of such interventions on long-term outcomes of clinical significance. Eysenbach et al113 cited lack of sufficient evidence to support use of peers for online programs. They suggested that research is required to evaluate specific conditions for which the effect of online PM might be maximized. A Cochrane review concluded that peer-led self-management programs may lead to small short-term improvements; it reported no evidence to suggest that these programs lead to significant long-term improvements in health-related outcomes.114
General conclusions about the effectiveness of PM based on review of clinical trials are limited for several reasons. These include the substantial variation in online mentoring programs, ambiguity about differentiation between mentoring programs and support groups, the variety of disease states, the severity of illness, and the variety of studied outcomes.
In contrast, our study was unique in several aspects and addressed some concerns about the effect of PM. For example, the peer mentors received formal training. We monitored the delivery of the mentoring program that proved relatively consistent. The disease state and severity of illness were well defined. Finally, the outcomes were distinct and measurable over a period of 18 months. Possible reasons for the superiority of online PM compared with FTF PM include convenient access without the restrictions of arranging for a meeting and flexibility of time of communication with less concern about imposing on the mentor's time. Furthermore, online communication allows for questions and answers to be presented in a less pressured setting, permitting time to think, as well as mutually more thoughtful communication.
Implications for Application to Other Chronic Diseases
Although certain aspects of the study are unique to CKD, and although the study benefited considerably from the already existing infrastructure of the KFCP and the PFPP, the protocol and results may be generalizable to other chronic diseases. Engaging patients, caregivers, and other stakeholders during the early phases is likely to produce important benefits to any patient-centered research study. Furthermore, and more specifically, engaging patients and caregivers by formally training them to be peer mentors is likely to improve patient-related outcomes.
The success of such programs will depend on cooperation among renal professionals, patients, caregivers, and other stakeholders, particularly patient advocacy organizations. In our study, we benefited considerably from collaboration with renal social workers for recruitment. Such programs and studies have their own unique challenges that need to be mitigated. For example, medical professionals may be concerned that the program will interfere with the patient-provider relationship.
Treatment Response Heterogeneity
We performed exploratory analyses to investigate HTEs with these results:
Among the online PM group, “not employed” status had a positive effect on the increased SF-12 PCS score, and being male had a positive effect on the increased SF-12 MCS score.
Among the FTF group, employed status had a positive effect on EKD and BKD scores.
Among the online PM group, married status and male sex had a positive effect on PAM scores.
Among the FTF PM group, unmarried status and female sex had positive effects on PAM scores.
Strengths and Limitations
The major strength of the study was the engagement of patients, caregivers, and other stakeholders throughout various stages. Stakeholders were involved in designing the study, recruiting participants, delivering the interventions, and disseminating the interim results to the community. Another strength was the relatively strong adherence to protocol and completion of the trial, although patients with stage 4 or 5 CKD have multiple highly severe comorbidities that might prevent them from participating in clinical trials lasting more than a few months.
Although the overall loss to follow-up was higher than expected, to minimize potential bias resulting from the effect of loss to follow-up, we used ITT analysis. The highest loss to follow-up occurred in the textbook-only (control) group, reducing concern about burden of intervention as the main reason for dropout. Loss to follow-up rates were similar between the 2 active intervention groups (ie, FTF PM and online PM).
Our study also had several limitations. First, we limited the participants to English-speaking individuals with computer literacy and internet access. Second, adherence to review of material by the textbook-only group was by self-report without monitoring by the study team. Third, although the program coordinator monitored adherence to the PFPP protocol, we did not collect information as part of the research, and we did not include frequency of contact with the interventions in the analyses.
Fourth, although the total number of participants included in the final analyses was sufficient per our power calculations, the number of participants belonging to certain subpopulations, such as rural and Hispanic patients, was limited, not allowing for exploratory subgroup analyses in those populations. Fifth, we conducted the trial in central Pennsylvania, limiting geographic generalizability. Sixth, because of the nature of the disease and its treatment, patients with CKD, particularly those undergoing hemodialysis, already belong to a community and are likely more willing than patients with other chronic diseases to engage actively in peer-related activities. Finally, the small number of patients using modalities of treatment other than hemodialysis did not allow for accounting for the effect of hemodialysis on outcome measures.
Future Research
As suggested by our findings, larger studies drawing participants from diverse backgrounds and geographic locales, as well as a larger number of patients with CKD not undergoing hemodialysis, will allow for more robust subgroup analyses. We concur with the recommendations from the Cochrane review114 of peer-led programs that future research should focus on assessing longer-term outcomes of interest to patients, such as repeated hospitalizations and satisfaction with treatment decisions. Other potential areas of research include assessing outcomes such as fatigue and cognition; examining relationships between health literacy and outcomes; and evaluating the role and end results of PM among children and adolescents, among patients with earlier stages of CKD, and among patients with other chronic disease states.
Because we used the existing infrastructure of our partnering organization, the KFCP, to deliver the interventions, our costs were limited to developing and maintaining the online platform and covering research staff salaries and participant stipends. Therefore, detailed cost-effectiveness studies of interventions that include PM are needed to help clarify the feasibility of such interventions in settings where a new infrastructure might be required. Finally, although we do not believe that the interventions in this trial were complex, using process evaluation to test these interventions is a potential area for future research.115,116